Overview
Dermatomes and myotomes represent segmental patterns of sensory and motor innervation from spinal nerves. Understanding these patterns is essential for neurological examination, spinal cord lesion localisation, radiculopathy diagnosis, and trauma assessment.
Use this summary together with spinal cord segments and nerve root pathways.
Dermatomes – Sensory Territories
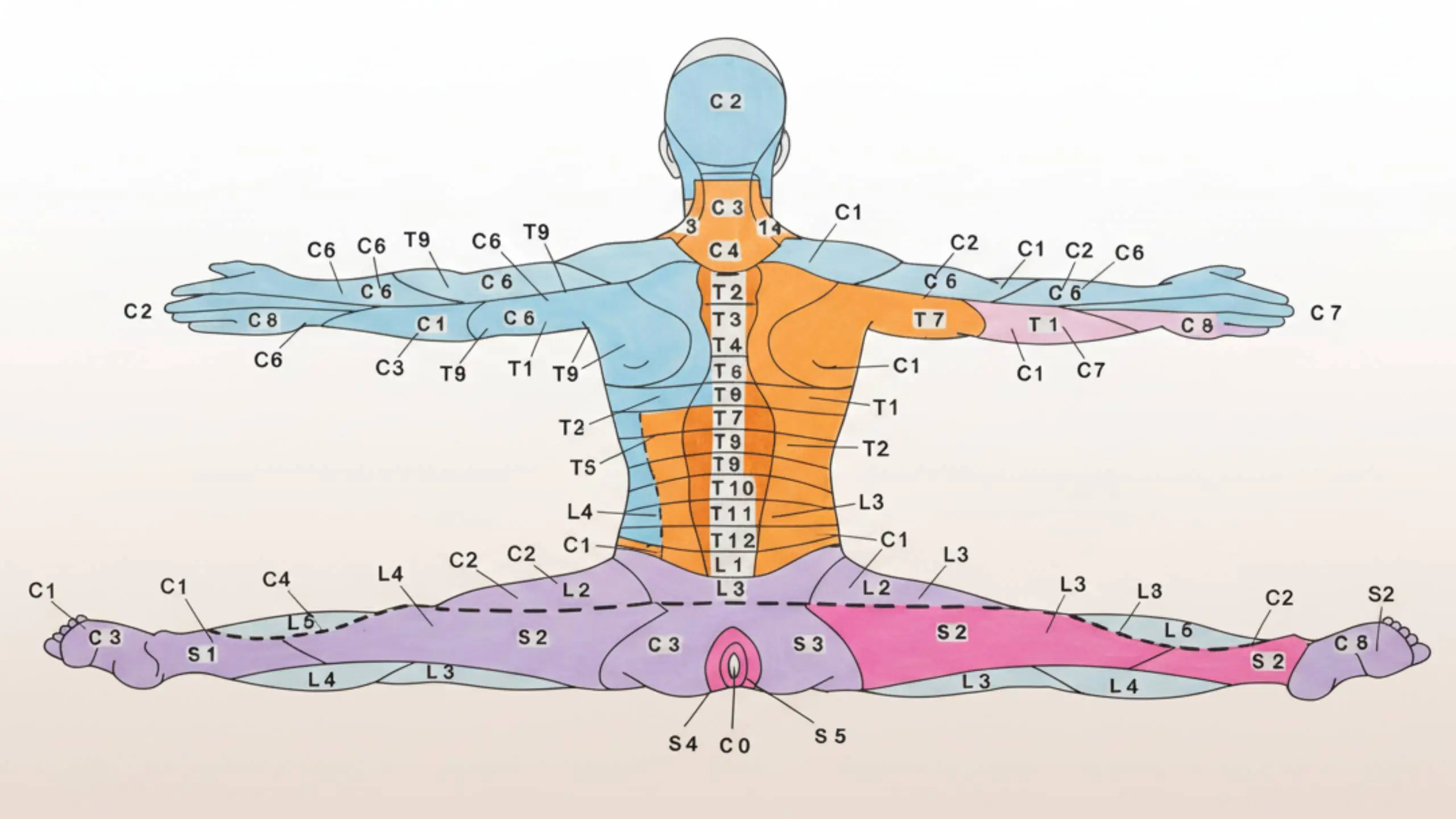
Each dermatome corresponds to an area of skin supplied by a single spinal nerve root. Clinical testing points help identify radiculopathy.
Cervical Dermatomes
| Root | Key Sensory Area | Clinical Notes |
|---|---|---|
| C2 | Posterior scalp | \"Greater occipital\" headache region. |
| C3 | Neck | High cervical collar region. |
| C4 | Shoulder cape | Phrenic nerve shares C3–C5 (diaphragm). |
| C5 | Lateral upper arm | Common in cervical radiculopathy. |
| C6 | Lateral forearm, thumb | Classic \"thumb numbness\" pattern. |
| C7 | Middle finger | Most common cervical radiculopathy. |
| C8 | Little finger, medial hand | Ulnar neuropathy mimic. |
Thoracic Dermatomes
| Root | Key Area | Clinical Notes |
|---|---|---|
| T1 | Medial forearm | Shares territory with ulnar nerve. |
| T2 | Axilla | Upper thoracic lesion marker. |
| T4 | Nipple line | Reference landmark. |
| T6 | Xiphoid region | Midline thoracic pain mapping. |
| T10 | Umbilicus | Classic emergency medicine reference. |
| T12 | Suprapubic region | Transition to lumbar dermatomes. |
Lumbar Dermatomes
| Root | Key Area | Clinical Notes |
|---|---|---|
| L1 | Inguinal region | Genitofemoral/ilioinguinal overlap. |
| L2 | Anterior thigh | Hip flexor pain distribution. |
| L3 | Medial thigh/knee | Patellar region involvement. |
| L4 | Medial leg, medial malleolus | Patellar reflex root. |
| L5 | Dorsum of foot, great toe | Most common lumbar radiculopathy. |
Sacral Dermatomes
| Root | Key Area | Clinical Notes |
|---|---|---|
| S1 | Lateral foot | Ankle reflex root. |
| S2 | Posterior thigh | Hamstring region. |
| S3 | Buttock crease | Pelvic floor sensory area. |
| S4–S5 | Perianal region | \"Saddle anesthesia\" in cauda equina. |
Myotomes – Motor Territories
Myotomes represent muscle groups controlled by a single spinal nerve root. Isolating actions helps identify root lesions.
For embryology context, see skeletal muscle development.
Cervical Myotomes
| Root | Key Action | Muscles |
|---|---|---|
| C5 | Shoulder abduction | Deltoid, supraspinatus |
| C6 | Elbow flexion, wrist extension | Biceps, brachioradialis, ECRL/B |
| C7 | Elbow extension | Triceps |
| C8 | Finger flexion | FDP, FDS |
| T1 | Finger abduction/adduction | Interossei |
Lumbar & Sacral Myotomes
| Root | Key Action | Muscles |
|---|---|---|
| L2 | Hip flexion | Iliopsoas |
| L3 | Knee extension | Quadriceps |
| L4 | Ankle dorsiflexion | Tibialis anterior |
| L5 | Great toe extension | EHL |
| S1 | Plantarflexion | Gastrocnemius/soleus |
| S2 | Knee flexion | Hamstrings |
Reflex Summary
Deep tendon reflexes correspond directly to specific myotomes.
| Reflex | Root Level | Notes |
|---|---|---|
| Biceps | C5–C6 | Primarily C5. |
| Brachioradialis | C6 | Forearm supination reflex. |
| Triceps | C7 | Classic C7 lesion test. |
| Patellar | L3–L4 | Primarily L4. |
| Achilles | S1 | Loss suggests S1 radiculopathy. |
Clinical Patterns to Remember
- C5: Shoulder abduction weakness; lateral arm numbness.
- C6: Thumb numbness; weak biceps/wrist extensors.
- C7: Triceps weakness; middle finger numbness.
- C8: Finger flexion weakness; little finger numbness.
- L4: Weak dorsiflexion; decreased patellar reflex.
- L5: Foot drop; dorsum of foot sensory loss.
- S1: Loss of ankle reflex; lateral foot numbness.
- Cauda equina: Saddle anesthesia (S2–S4), urinary retention.
For pathway and maps, review nerve roots and spinal cord segments, plus upper limb dermatomes.